On incidental findings

Nikhil from Out of Pocket recently wrote an essay about incidentals in cancer screening that I thought was measured and well documented. Given that I run a startup that offers the types of Full Body MRI scans Nikhil describes, I wanted to provide my perspective on the risks (and benefits) of such scans.
First off – disclaimer. I’m obviously biased as I’m very invested in this space. I’m the Founder & CEO of Ezra, a company that offers cancer screening solutions powered by Full Body MRI and Artificial Intelligence. I started Ezra because I am personally at high risk for cancer, and because I lost my own mother to metastatic cancer. Had my mother’s cancer been diagnosed early, she would likely still be alive now. How do I know that? Data.
Early detection saves lives
Leaving incidentals aside for a moment (I’ll come back to the topic shortly), the first question we need to answer is: does detecting cancer early lead to better outcomes? According to the American Cancer Society (page 21), here’s what five-year survival rates look like by stage at diagnosis:
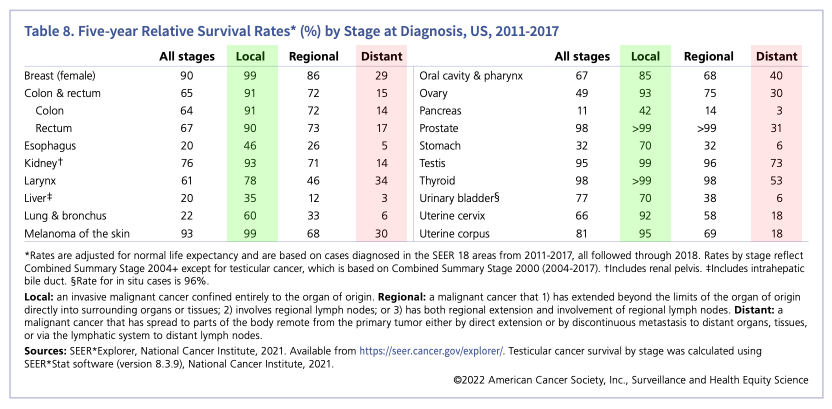
Undoubtedly, finding cancer early increases survival rates. Let’s take kidney cancer for example: it has a 93% 5-year survival rate if detected at stage 0-1 (local), and a 14% 5-year survival rate if detected at stage 4 (distant). That’s a 600% improvement in survival rate for early detection vs. late detection.
And it’s not just the survival rates, it’s also the costs. The national cost of cancer care in the US is over $200 billion, and most of it is end-of-life care in the last 4 months of a cancer patient’s life. That’s because over 50% of all cancers are detected late, and treating late-stage cancer is 2 to 4 times more expensive than early-stage, according to the World Health Organization.
But Nikhil’s point, and he’s right to raise it, is this: “Yeah Emi, but for every person who finds kidney cancer early using an MRI, 10 people will go through unnecessary downstream procedures such as biopsies - some might even die from them.”
And he’d be right. Kind of. The thing is, it depends on what you do about these incidental findings. If you indiscriminately follow up each of these rabbit holes, of course you will do more harm than good.
But it’s not what should be done, and it’s not what we do at Ezra. So I’d like to provide a bit of clarity on how we think about incidental findings, and talk about the framework we’ve put in place to ensure that first, we do no harm.
Before we jump in I’ll also note that we’ve developed this methodology alongside some of the world’s leading medical experts, and we’re confident it will enable us to ultimately make Full Body MRIs standard of care.
Provide clarity and guidance
Typically, after you get an MRI scan you receive a radiology report and that’s about it. “Hey Emi, you have a 3-cm focal nodular hyperplasia in your liver, good luck!”
That’s not what we do at Ezra. We’ve created an AI, Ezra Reporter, that has been trained on a proprietary dataset of thousands of radiology findings, their meaning, and what the next steps should be for each individual finding. So for every single radiology impression in an Ezra scan, we provide a translation of what it means and what you should do about it.
Here’s our “focal nodular hyperplasia” finding, as it’s typically written in an Ezra report:
“Focal nodular hyperplasia (FNH) is a benign (non-cancerous) lesion that consists of liver cells surrounding a central scar. While the exact cause of FNH is unknown, it is thought to occur as a response to arterial malformations (either acquired or present at birth) within the liver. FNH is the second most prevalent liver lesion (the first being hemangioma), usually found incidentally on imaging, and typically does not cause symptoms or require treatment. When symptoms are present, the most commonly reported symptom is abdominal pain and if persistent, requires surgical treatment.
While this lesion most likely represents FNH, other liver lesions (e.g. hepatocellular adenoma) may have a similar appearance so further imaging is needed.”
This is much more clear than the typical radiology impression. It explains what an FNH is, how prevalent it is, and what you should do about it. Our AI creates these translations for every single type of finding in an Ezra scan. If you’re curious to see a full Ezra report, you can view a sample here.
Furthermore, every Ezra member gets to speak with one of our on-staff medical providers, led by our incredible Medical Director, Dr. Carol DerSarkissian.
Non-invasive follow-up and longitudinal monitoring
We have found that providing clear, concise Ezra reports alleviates most concerns people have about incidentalomas. But how about findings that are indeterminate? Things that might be cancer, might not, and require follow-up or monitoring.
We’ve developed a methodology at Ezra that has enabled us to successfully scale Full Body MRIs to thousands of people without any significant downstream negative effects. This methodology has three components - a scoring system, longitudinal monitoring, and non-invasive personalized follow-up. It’s the first time we talk about the framework publicly at Ezra, so I’ll expand on all three.
E-SCORE
First, every single finding in an Ezra scan gets ranked by our AI (and signed off by our medical providers) on a scale of 1 to 5, with 1 being just informative, 5 being critical and emergent. We modeled it after the American College of Radiology’s RADS system (PI-RADS, BI-RADS, etc.).
Depending on a finding’s E-SCORE, we determine what should be done about it, and we have two tools in our toolbox:
Longitudinal monitoring
Our thesis at Ezra is that longitudinal monitoring of an individual’s body is the best way to detect cancer early, while minimizing unnecessary follow-up. The urgency of potentially-harmful follow-up procedures decreases significantly if you have previous scans to look at for an individual, and if you know that the person will be scanned again at regular intervals.
Radiologists looking at Ezra scans will compare any concerning findings to what may be found on a member’s previous scans. The lack of change from one scan to another in itself rules out many concerning conditions. Prostate cancer, for example, is generally a slow-growing cancer, so what is concerning is not its presence (most men will have it at some point in their lives), but any sudden change in its appearance.
Most findings in a typical Ezra scan receive an E-SCORE of 3 and below. These don’t get any kind of follow-up, they just get monitored over time using an annual Ezra scan. Because MRI scans don’t use ionizing radiation, members can safely get a scan every year without any negative health effects.
Our Scientific Advisor Dr. Dan Sodickson, the inventor of parallel imaging in MRI and the Chief of Innovation in the Department of Radiology at NYU Grossman School of Medicine, did a fantastic job laying out our approach in this video on Huge if True by Cleo Abram. It’s worth a watch:
Longitudinal monitoring is especially important for cancers such as prostate cancer, where you want to avoid unnecessary prostate biopsies (Nikhil does a great job laying out how unpleasant prostate biopsies are). With Ezra, you can get a 20-minute Prostate MRI every year to monitor how your prostate cancer is developing, and determine whether it’s becoming more aggressive. No needles, no biopsies, no pain. Half an hour per year.
Even further, we’ve developed the first FDA-cleared Prostate AI, that makes it easy to measure and monitor prostate findings over time.
Non-invasive follow-up
Finally, Ezra E-SCOREs of 4 and 5 generally require follow-up. Our approach is to always recommend a follow-up diagnostic scan of the organ of interest prior to any invasive procedure such as a biopsy. For the liver, that might be a liver MRI with contrast. For thyroid, it might be an ultrasound. And so on. This is where most follow-up investigations end.
I have had to go through one of these procedures myself. In my very first Ezra scan a few years ago, we discovered an indeterminate liver lesion. Our medical team recommended that I do a follow-up diagnostic MRI scan with contrast, which I did. The diagnostic scan determined that my lesion is a focal nodular hyperplasia, so nothing to be concerned of. I have been tracking it with my annual Ezra scan for the past few years and it has not changed in size. The combination of non-invasive follow-up and longitudinal monitoring has given me great peace of mind that this isn’t cancer.
Multi-modality screening
Our focus at Ezra is on leveraging MRI and Artificial Intelligence to detect cancer early, but there are other endeavors that are also showing promise. Most notably, ctDNA-based liquid biopsies have shown some encouraging results, and I’m excited about how this space develops.
What’s interesting about liquid biopsies is that they have very high specificity but very low sensitivity, especially for early-stage cancer. Comparably, MRIs have very high sensitivity, with lower specificity (there’s always a trade-off between the two).
Now, if you were to combine the two tests, that could be pretty powerful. So I think the future of cancer screening is multi-modality. At Ezra we incorporate low-dose CT scans (for lung cancer screening) and mammograms (for breast cancer screening) alongside our Full Body MRI. I’m really excited about adding more modalities to our protocol in order to increase overall coverage as well as our sensitivity & specificity.
Furthermore, in addition to multi-modality screening, I’m excited about using AI to develop more accurate predictive models (and better scans) that take into account regular, longitudinal data for an individual. This is an area we are actively pursuing at Ezra – we’ll have some news on this front in the near future.
The future of cancer screening
I’m really happy that Nikhil is using his platform to create a conversation around cancer screening, and bringing up the potential pitfalls of these new tools and technologies available to us.
Personally, I believe we have a cure for cancer - it’s early detection. At Ezra we are driven by an unwavering ambition to detect cancer early for everyone in the world, and I’m hoping this article shows how much effort our team is putting into doing the right thing for our members.
In Health,
Emi Gal
Founder & CEO
Ezra
Thank you to Dr. Carol DerSarkissian, Dr. Dan Sodickson, and Dr. Oguz Akin for reading drafts of this.