The Path to 100 Healthy Years

Our mission at Function is to help everyone in the world live 100 healthy years. For the past few months, my team and I have been asking one question: is it possible for the average population (not the outliers) to live 100 healthy years, and what would it take to get there? Let's dive in.
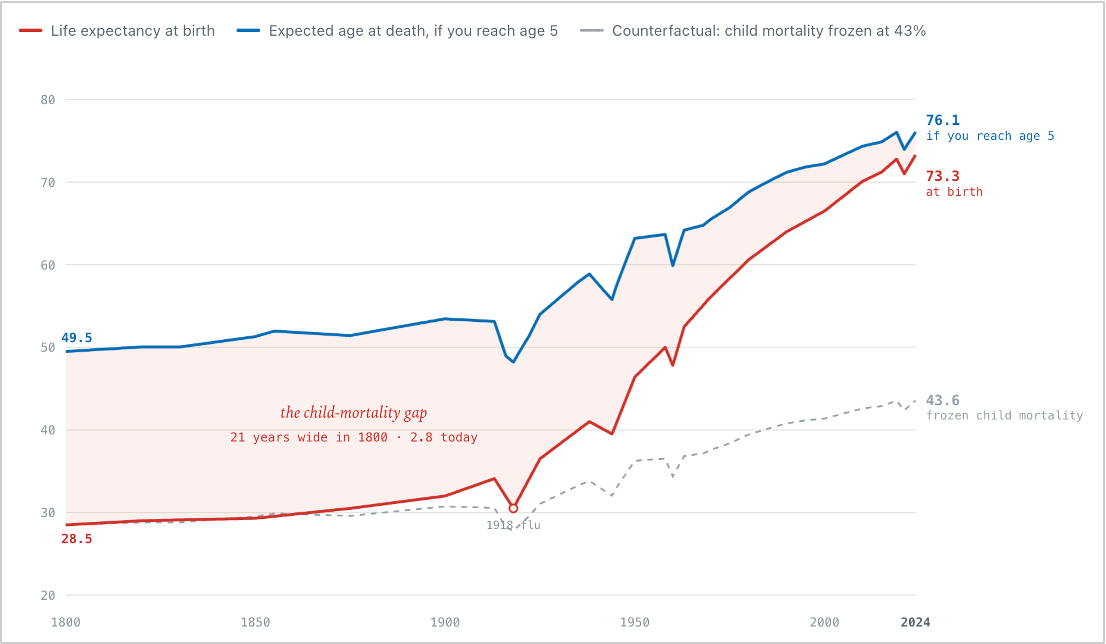
We're living much longer than we used to. In the 1800s, the average life expectancy was 29. By the 1950s that had climbed to 46, and today it's roughly 73 years worldwide. We've more than doubled the average human lifespan in a little over a century – an extraordinary accomplishment worth understanding in a bit more detail.
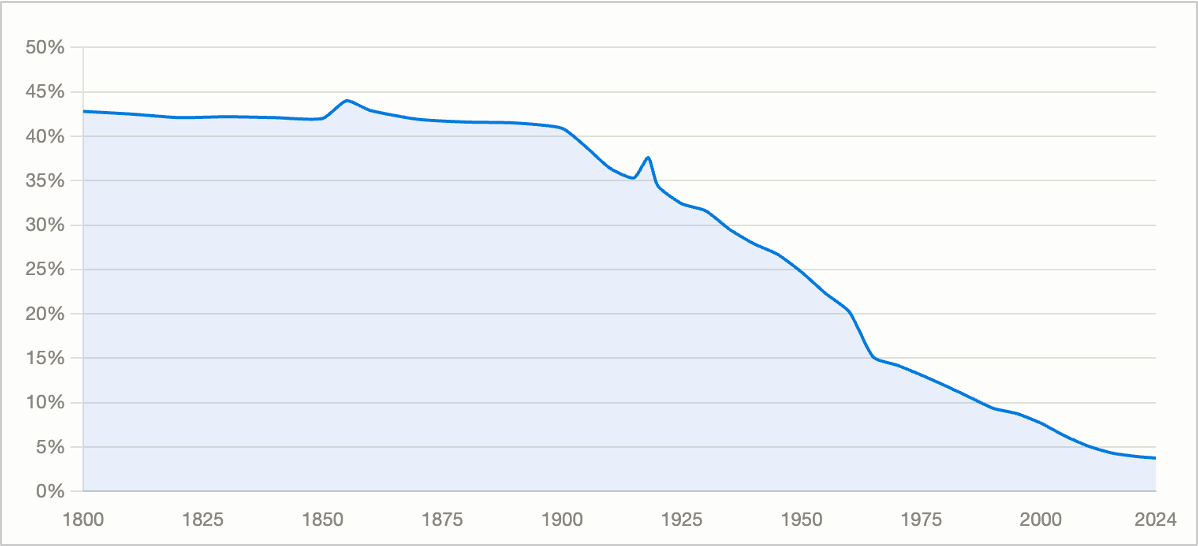
A big chunk of our life expectancy gains came from solving child mortality. In the 1800s, close to half of all children died before the age of five. Today it's under 5% worldwide thanks to clean water, hygiene, vaccines, and antibiotics.
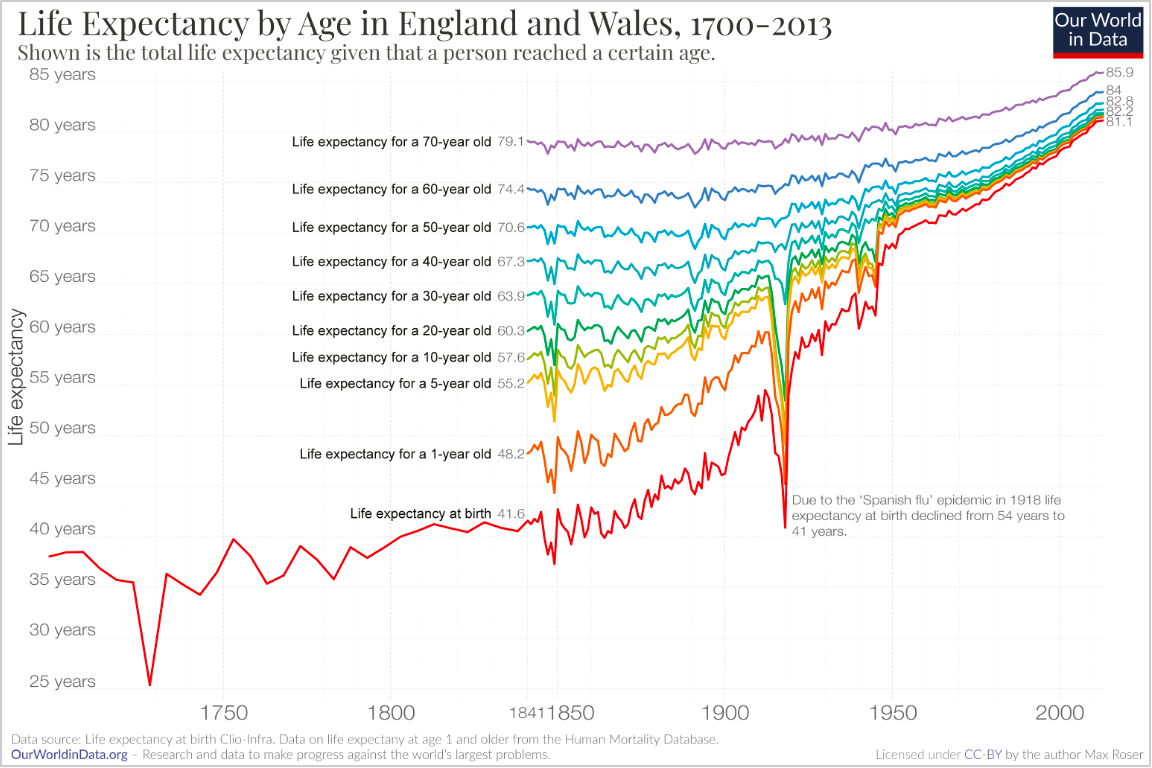
Fixing child mortality did much of the work behind the headline life expectancy numbers. However, even if you remove child mortality entirely, we've still added 26 years of lifespan across all ages. A 70-year-old in the 1800s could expect to live to 79; today that same person would live to 86. We got better at keeping adults alive, not just kids.
We live significantly longer. What kills us has also changed completely over the last century.
From roughly 1915 to 1945, the main killer across almost every age group was infectious disease – tuberculosis, pneumonia, measles. We beat those back with hygiene and antibiotics, people started living longer, and heart disease took over as the leading killer of adults from the 1940s through the 1990s.
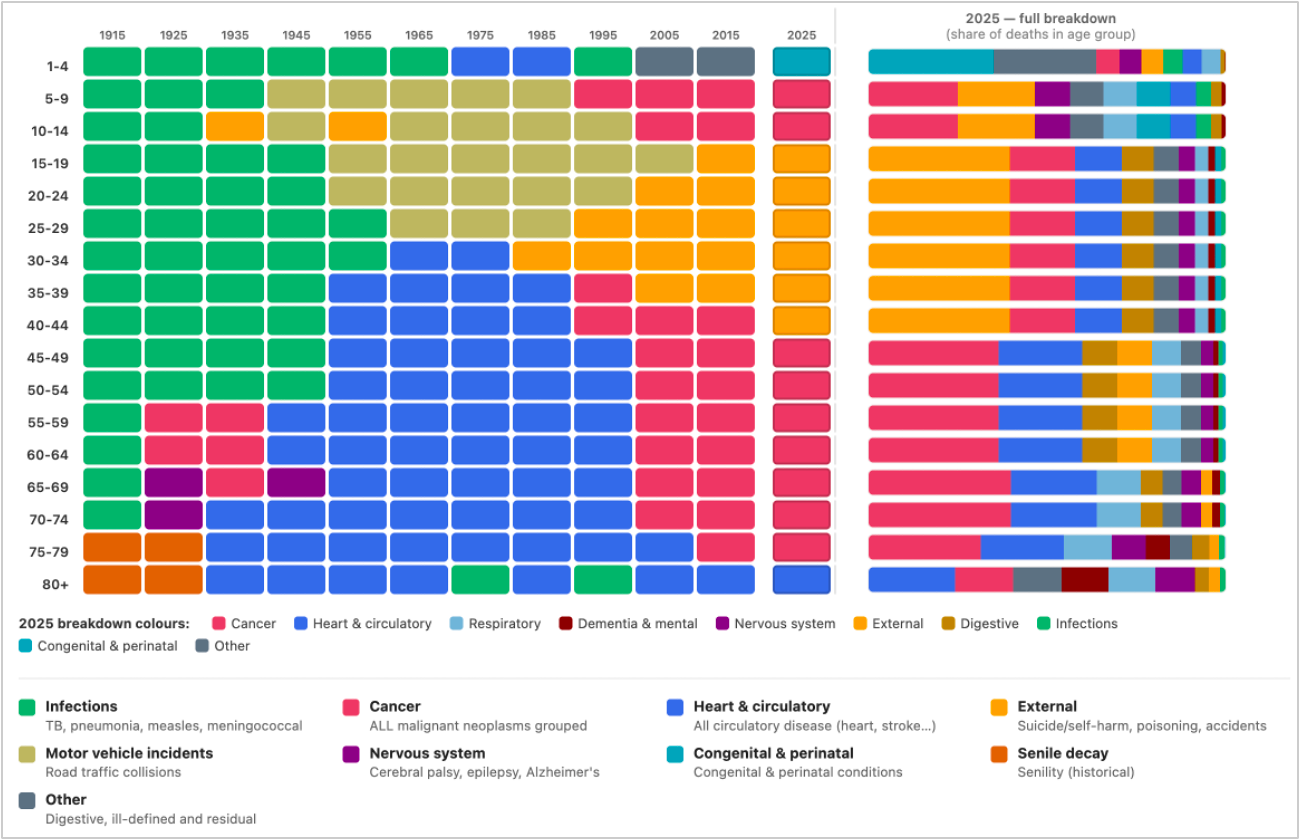
Heart-disease death rates peaked around 1968 and have been falling for the past few decades. Less smoking, better blood-pressure control, and improved cardiac care drove most of it, with statins adding to the trend starting the 1980s. Heart disease remains the leading cause of death in the US, though cancer has passed it in some states and age groups (source).
As of 2025, the picture splits pretty cleanly by age. For people aged 15 to 40, the leading cause of death is now drug-related – overdoses, mostly opioids and fentanyl (source). Over the age of 40, it's cancer and heart disease. And past 80, dementia joins them.
So it really all comes down to three diseases: cancer, heart disease, and dementia. One in three of us will be diagnosed with cancer in our lifetime. By middle age, roughly two-thirds of apparently healthy adults already have subclinical plaque. One in ten will develop dementia by age 80 (source, source, source).
The good news is that cancer, heart disease, and dementia are all addressable with a combination of early detection, lifestyle, and pharmacological interventions.
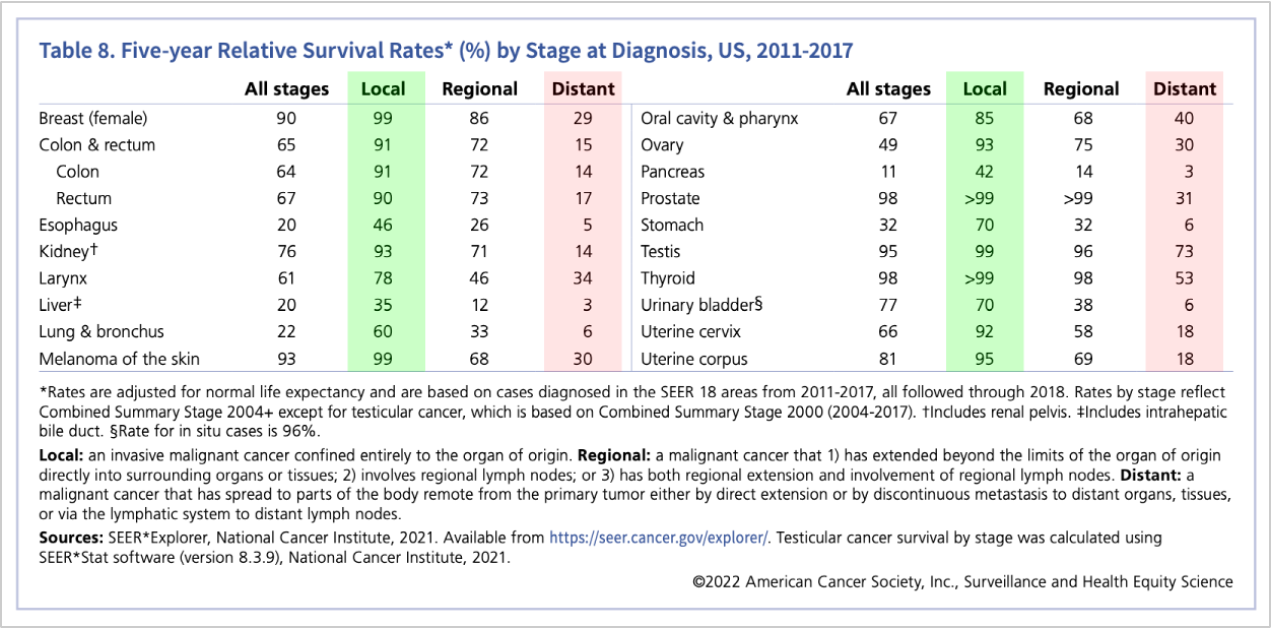
Cancer is largely non-lethal if you catch it early. Looking at the five-year survival rates makes this crystal clear across every type of cancer. Pancreatic cancer caught early (localized) has about a 42% five-year survival rate; caught late, around 3% – a more than tenfold difference. Breast cancer has a 99% survival rate when found early versus 29% late. The pattern holds across nearly every type of cancer. Finding cancer early is the difference between a manageable problem and a death sentence, and survival comes down almost entirely to stage at diagnosis.
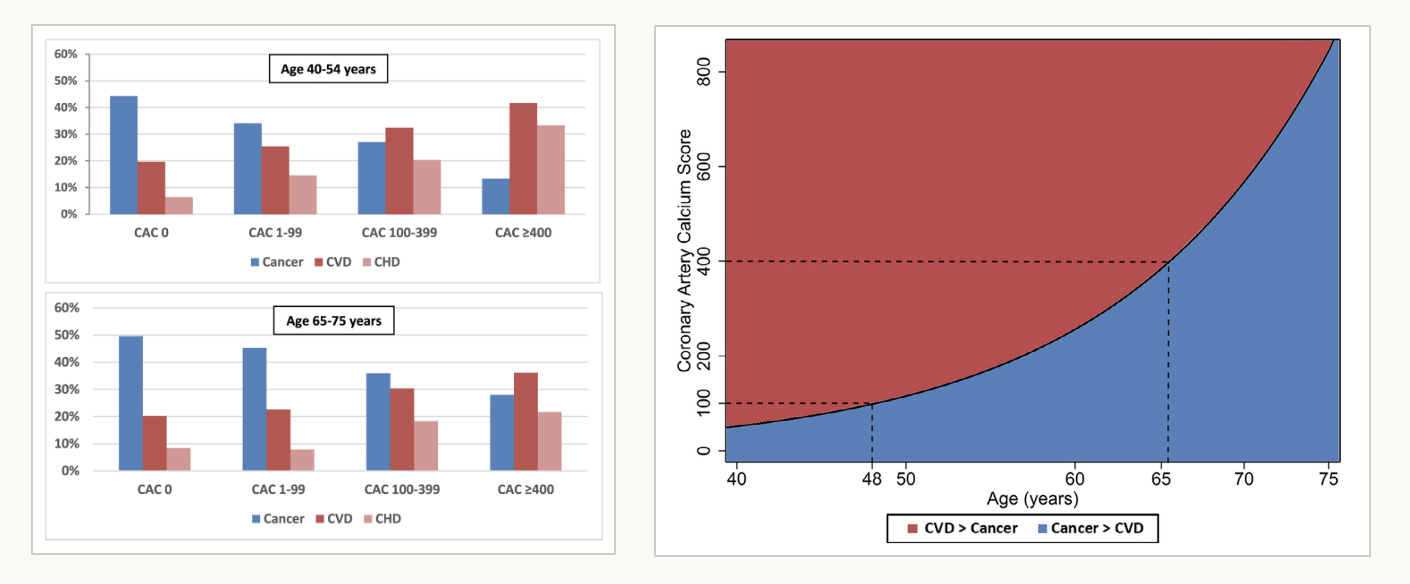
Heart disease is largely preventable. The chart below shows cause of death by age, split by whether a person's coronary calcium score (CAC) is zero or above. Your CAC is essentially a measure of how much calcified plaque has built up in your coronary arteries, narrowing the arteries and preventing proper blood flow to the heart. In both the 40 to 54 and 65 to 75 age groups, a score over 400 sharply raises the risk of dying from a heart attack rather than cancer.
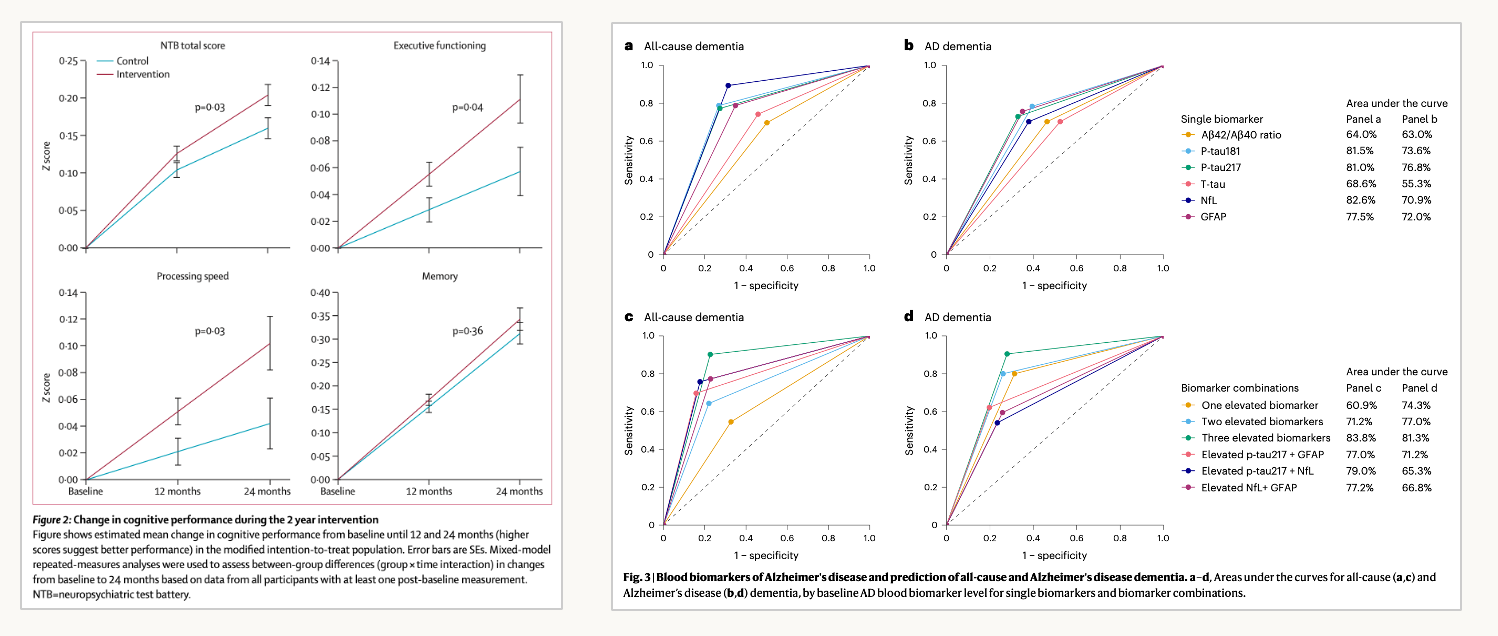
Dementia can be delayed. We can't fully prevent dementia or Alzheimer's yet as we don't understand them well enough. There is, however, growing evidence that a combination of cognitive training, lifestyle changes, and diet can delay dementia's effects on executive function, memory, and processing speed. You just need to start early (source).
The common thread across these three diseases is early detection, which brings us to my proposed protocol for not dying young.
I think about staying alive in five buckets: data, exercise, diet, supplements, and pharmacological interventions. This post focuses on what we can do to prevent the three big killers: cancer, heart disease, and dementia; I've written in more detail about my personal longevity protocol here.
Data
Let's start with data, as you can't act on what you can't see. For each of the three killers, there's a small set of things worth testing.
For heart disease, three numbers matter most. The first is your coronary calcium (CAC) score, from a quick chest CT that measures how much calcified plaque has built up around your coronary arteries. CAC is most useful at the extremes. A zero, at the right age, is reassuring as it means you're far more likely to die of something other than heart disease. A high score (400+) is a real red flag. CAC scans are cheap, and everyone over 40 should get one (we offer them at Ezra).
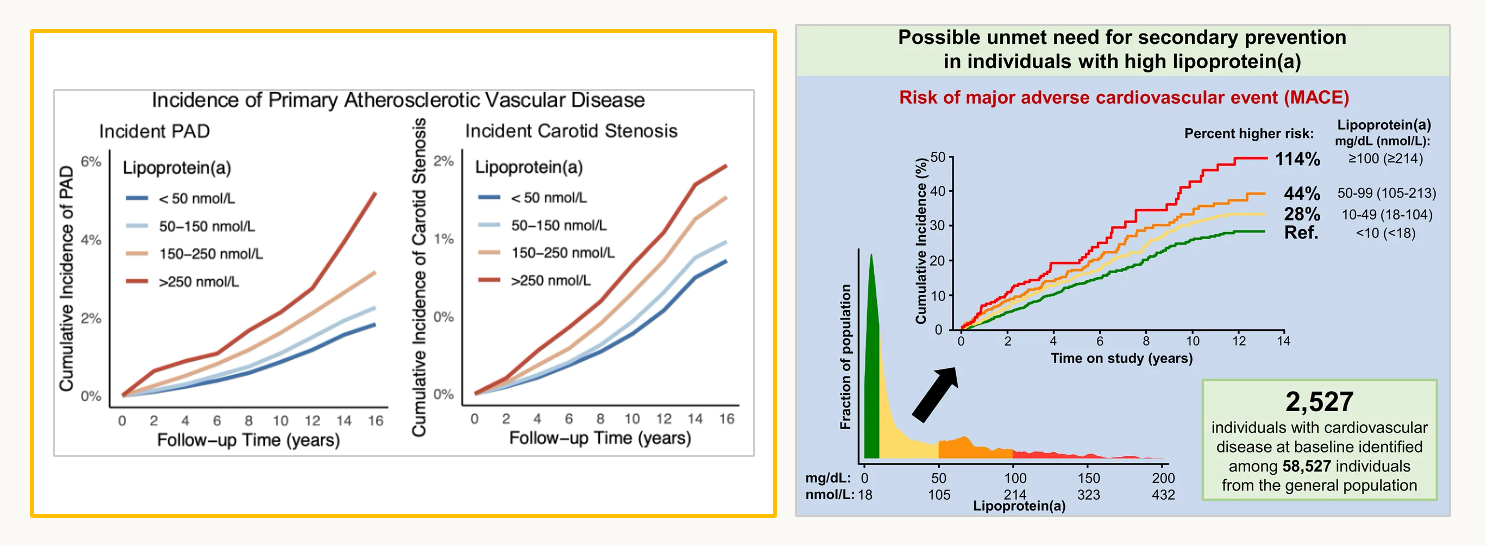
The second, a marker almost nobody talks about, is Lp(a), a lipoprotein that rides along with your LDL and is mostly set by your genes. A high Lp(a) of over ~250 nmol/L can more than double your heart-disease risk. It rarely gets tested and barely changes over your life, so measure it at least once (source). We offer Lp(a) testing at Function.
LDL matters too. Lowering it reduces cardiovascular risk at nearly every age – it's now well established that lower LDL leads to fewer cardiovascular events (source).
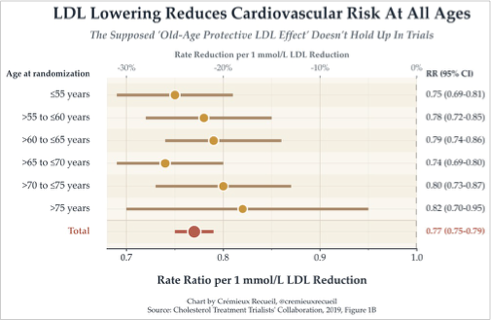
Lowering LDL reduces the risk of a cardiovascular event even when Lp(a) stays constant. Ezetimibe, a drug that lowers LDL but does nothing to Lp(a), still reduced cardiovascular events in a randomized trial. That tells you LDL and Lp(a) stack as independent risks (source).

For cancer, the big problem is that we only have screening tools for a handful of organs: breast (mammogram), lung (low-dose CT), cervix (pap smear), prostate (PSA, a pretty bad test in terms of sensitivity & specificity), and colon (colonoscopy). These account for about half of all cancer cases but only 35% of cancer deaths. The organs that kill you — pancreas, liver, brain, kidney, ovaries, etc., are the ones we can't routinely screen, so cancer there usually isn't found until symptoms appear.
This gap is why I built Ezra: it screens the organs you otherwise couldn't, using the fastest, most advanced full body MRI in the world. Because MRI uses magnetic resonance rather than ionizing radiation, you can safely scan every year and track changes over time — so something new that's growing across scans looks very different from something that's sat unchanged for three years. The biggest deterrent to these scans is the real risk of incidental findings – I've written about how to deal with that at length here.
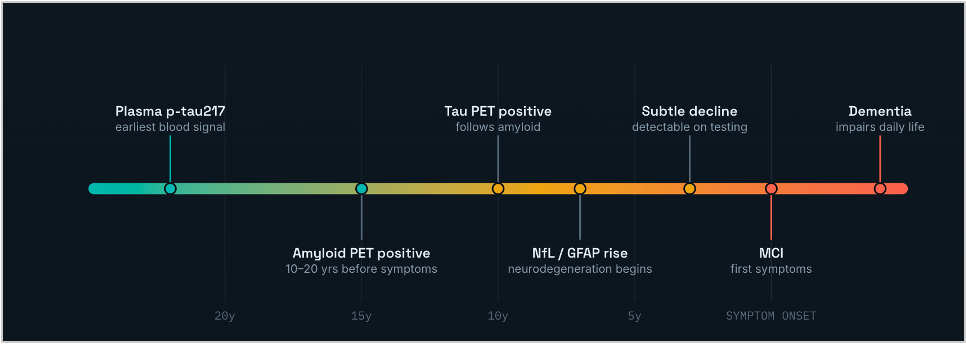
For dementia, there is now a protein marker called p-tau217 that, in studies, predicts dementia risk more than 20 years before symptoms appear (source). We offer it as a blood test at Function.
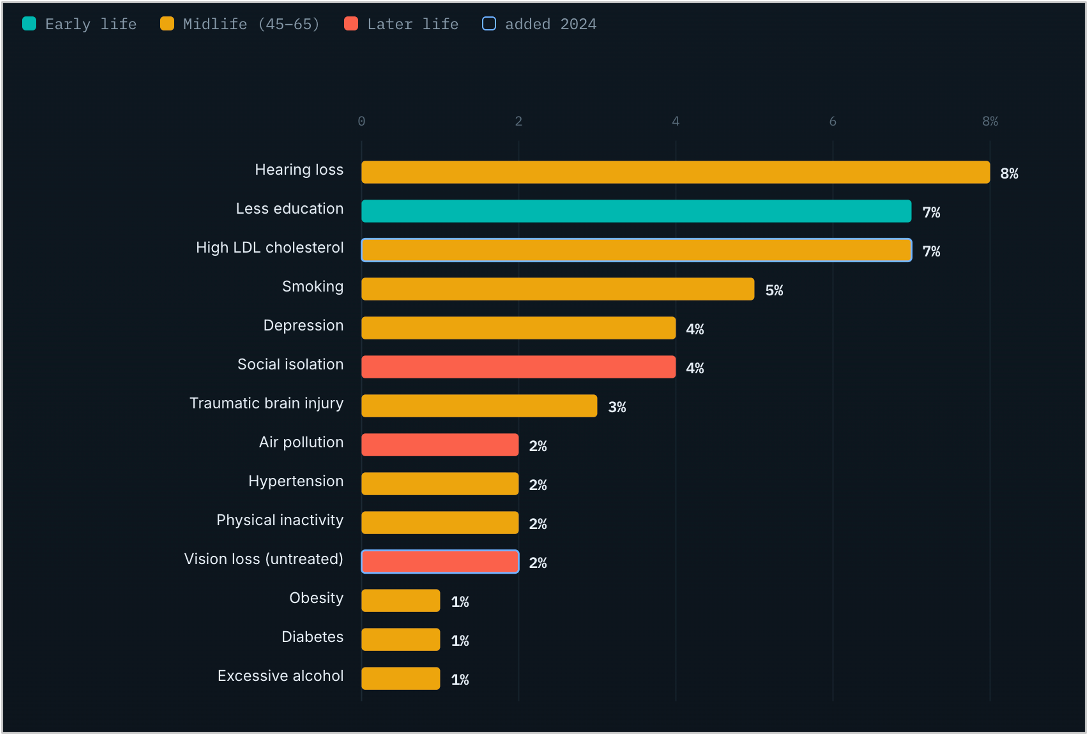
We also understand relatively well what increases our risk for dementia, and there are a number of risk factors you can act on: hearing loss, high LDL, smoking, depression, pollution, and more (source).
Exercise
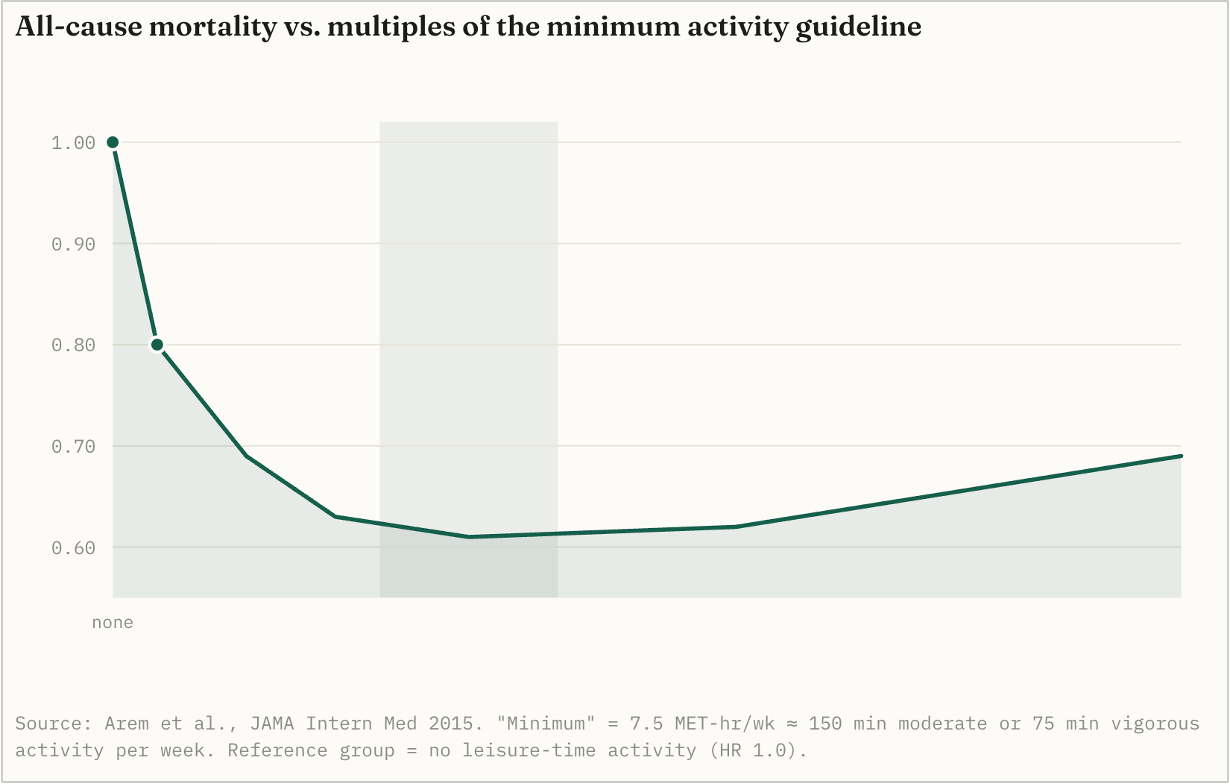
The most powerful longevity drug is exercise. If you only do one thing on this list, exercise. Plot all-cause mortality against how much someone exercises per week and the drop is enormous: moving regularly can cut your risk of dying by 30%. No drug on earth does that. The sweet spot is around 150–200 minutes of moderate activity a week, but the single biggest jump comes the moment you go from nothing to something.
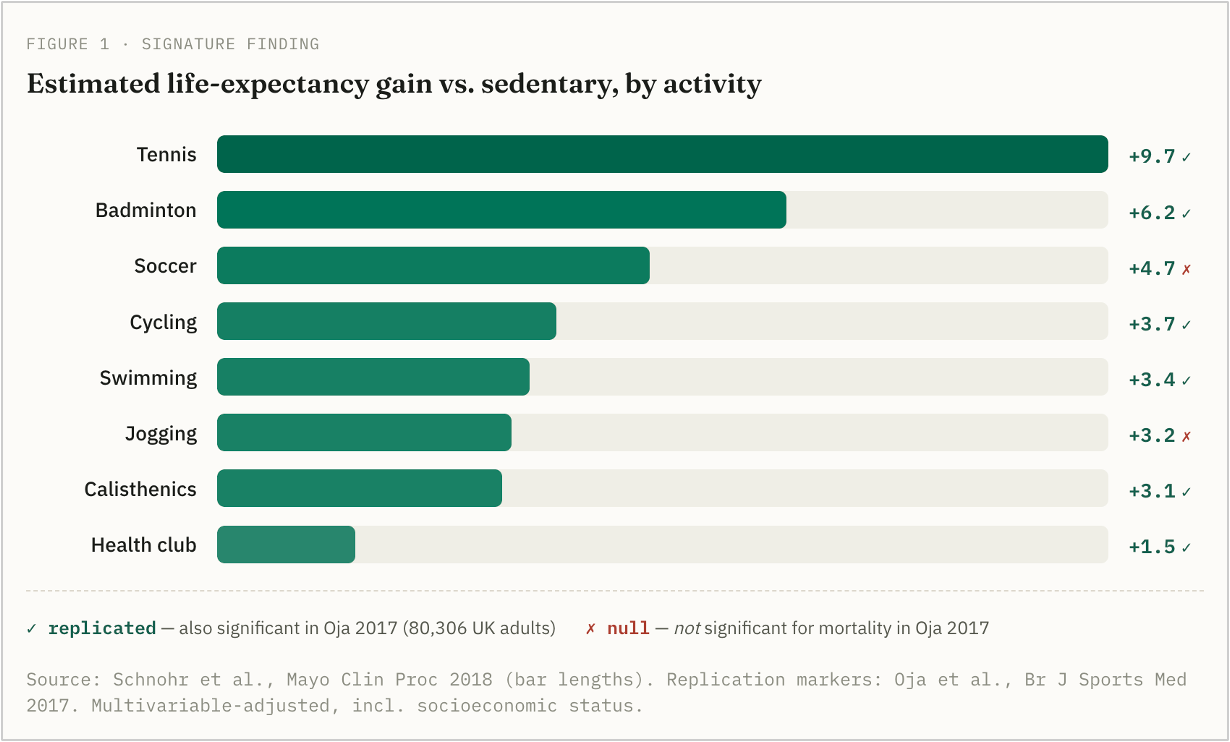
Which exercise you choose matters too, though I'd hold the data below loosely. Across multiple observational studies, tennis showed the largest longevity gain, on the order of 9.7 extra years. I assumed this was confounded by wealth (rich, healthy people play tennis), so I dug in; at least one study adjusted for socioeconomic status and the effect held. It's observational, not a randomized trial, so don't take the exact number too literally. The real takeaway is that almost any sport buys you years.
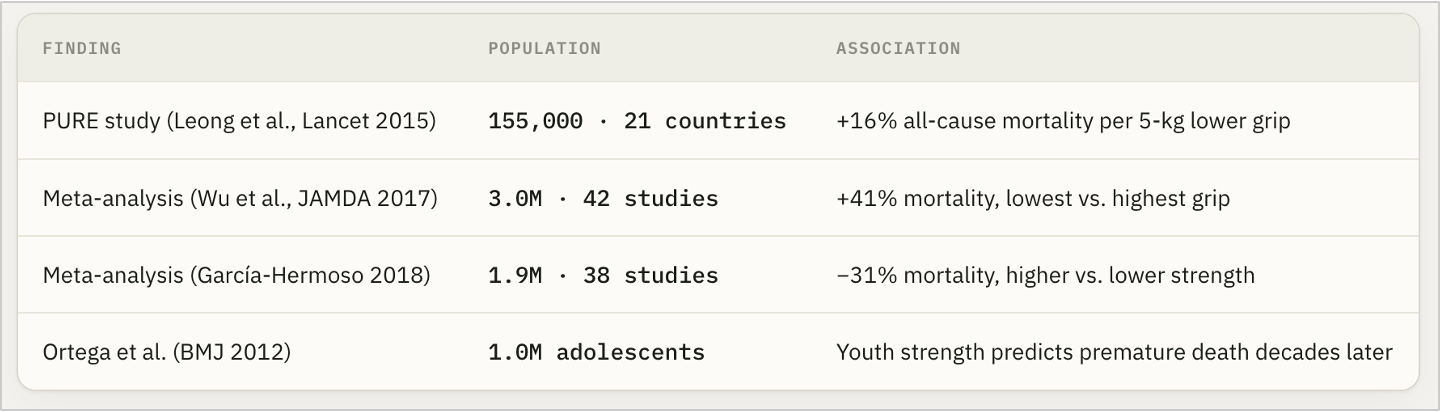
Strength matters as well, and grip strength turns out to be one of the cleanest proxies. In a study of roughly 140,000 people, each 5kg drop in grip strength was linked to about 16% higher all-cause mortality. So lift to get strong. If you end up lifting extremely heavy – do not, under any circumstances, ever take steroids. A couple of studies have shown that anabolic steroids increase mortality rates (source, source).
Diet
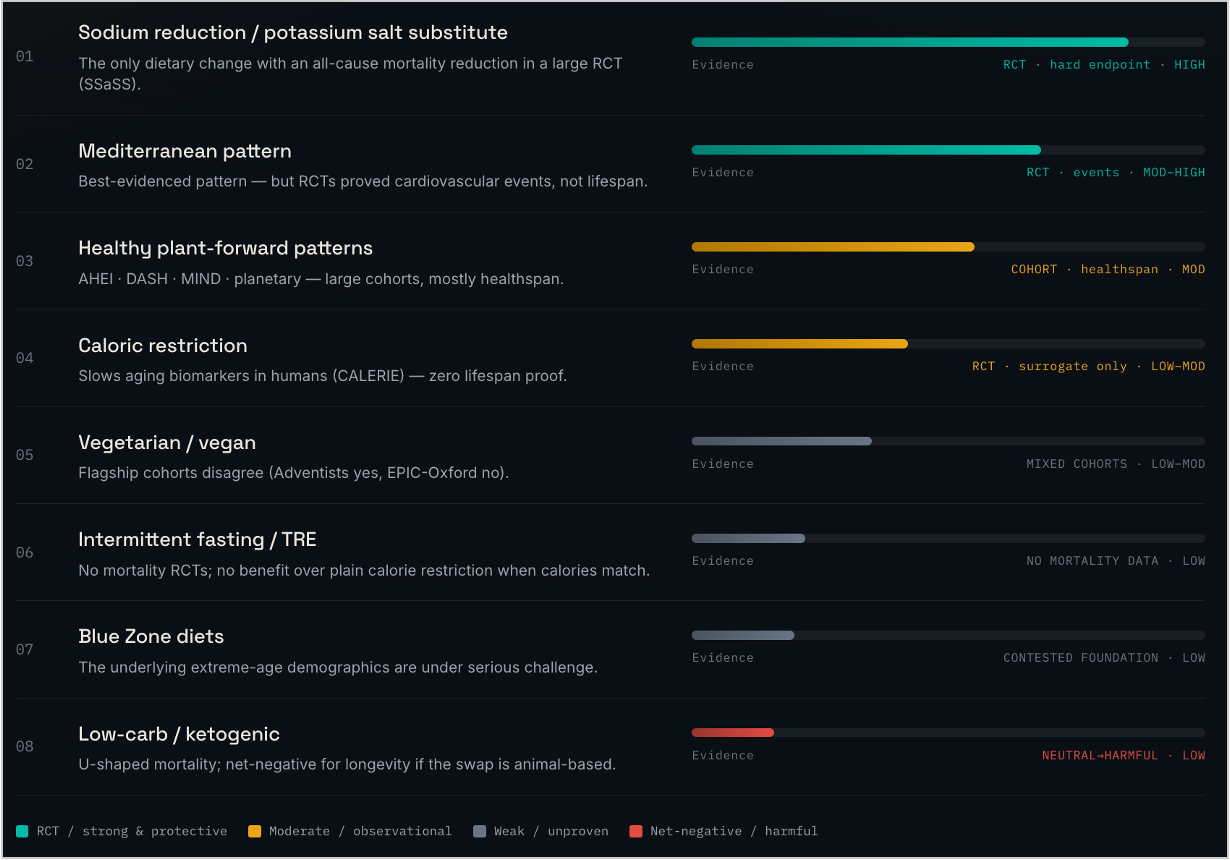
Many randomized control trials have been run on diet, with very promising results. There are at least two dietary randomized trials with statistically significant results – one on cutting salt, one on the Mediterranean diet. Both showed a 15-20% reduction in all-cause mortality, and a whopping 30%+ reduction in cardiovascular-related deaths. What we eat matters!
My rule on the diet front is boring on purpose: go easy on salt, eat mostly whole foods and vegetables with some fish, nuts, and olive oil; don't overeat. The Mediterranean approach works largely because it's barely a diet — there's nothing extreme to rebel against, so anyone can stick with it long-term.
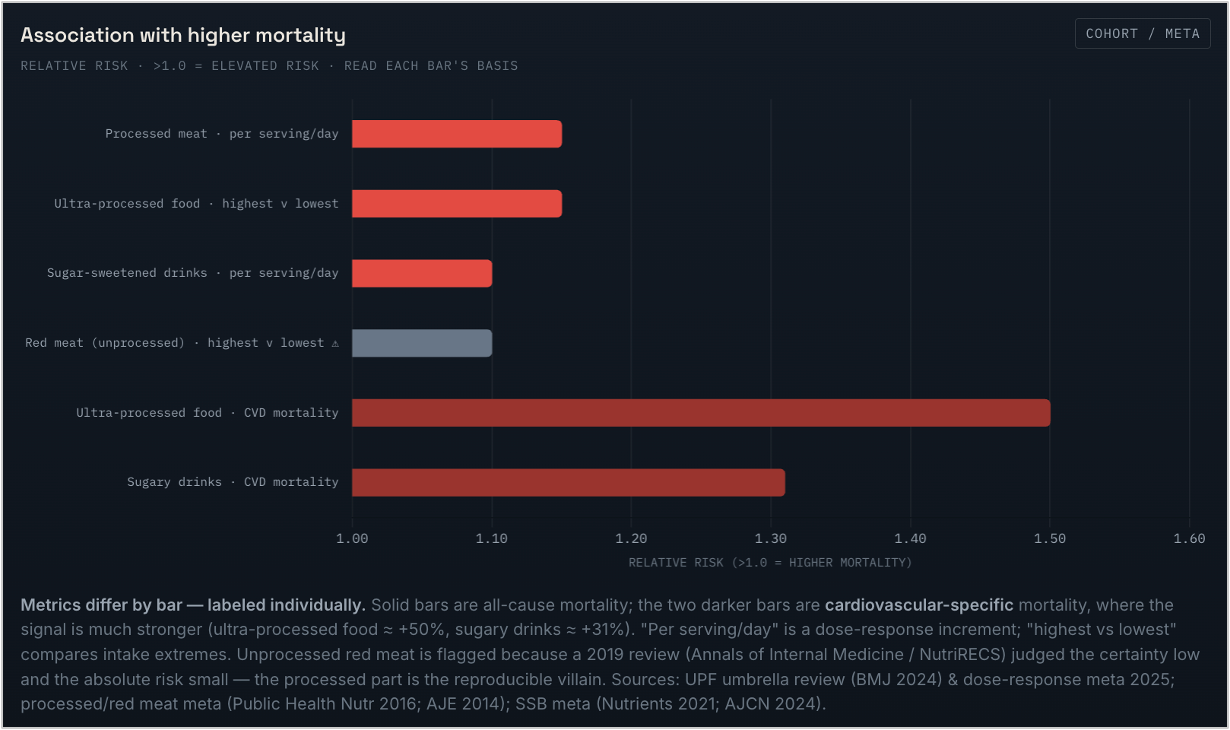
The clearer signal is what to remove. Processed meat, ultra-processed food, and sugar-sweetened drinks all track with higher mortality, and the latter two specifically raise cardiovascular death. Processed meat is now classified as a carcinogen in the same category as tobacco. That should tell you how to feel about it.
Alcohol
For years the story was that a drink or two a day is good for you; the famous J-curve, where moderate drinkers outlived teetotalers, supposedly because alcohol nudges up your HDL. That story is now dead. The curve was an artifact of who ends up in the "non-drinker" bucket: it's full of people who quit because they got sick (the "sick-quitter" problem), and moderate drinkers tend to be richer, leaner, and more active to begin with. Clean that up in the bias-corrected data and the survival benefit at low intake disappears (source). The cleanest evidence comes from Mendelian randomization, which uses gene variants that affect how much people drink as a natural randomized trial. Do that and the J-curve flattens into a straight, upward line (source).
So where does that leave us? Heavy drinking is unambiguously bad – all-cause mortality climbs up, and it's one of the top killers of people under 50. Moderate drinking is subtler. Once you correct for the biases above, a drink or so a day doesn't clearly shorten your life in the all-cause mortality numbers. But, and this is the correction to the old narrative, it's definitely not buying you years. The wine isn't extending your life; if anything the level that minimizes total health loss is zero (source).
And alcohol is definitely not risk-free, even in moderation. First, because of cancer: alcohol is a Group 1 carcinogen, same evidence tier as tobacco, meaning it causes cancer. The risk starts from the very first drink, with no safe threshold. Breast cancer risk rises ~7–10% for every daily drink (source), and roughly 1 in 7 alcohol-attributable cancers worldwide occur at light-to-moderate intake (source). Second, cardiovascular: the same genetic studies that killed the J-curve show alcohol raising blood pressure, stroke, and coronary disease in a straight line, with no protective dose (source). So my read: don't panic about the occasional drink, but drop the idea that it's doing anything good. If you drink, less is better – you're spending a little health, not banking it.
Supplements
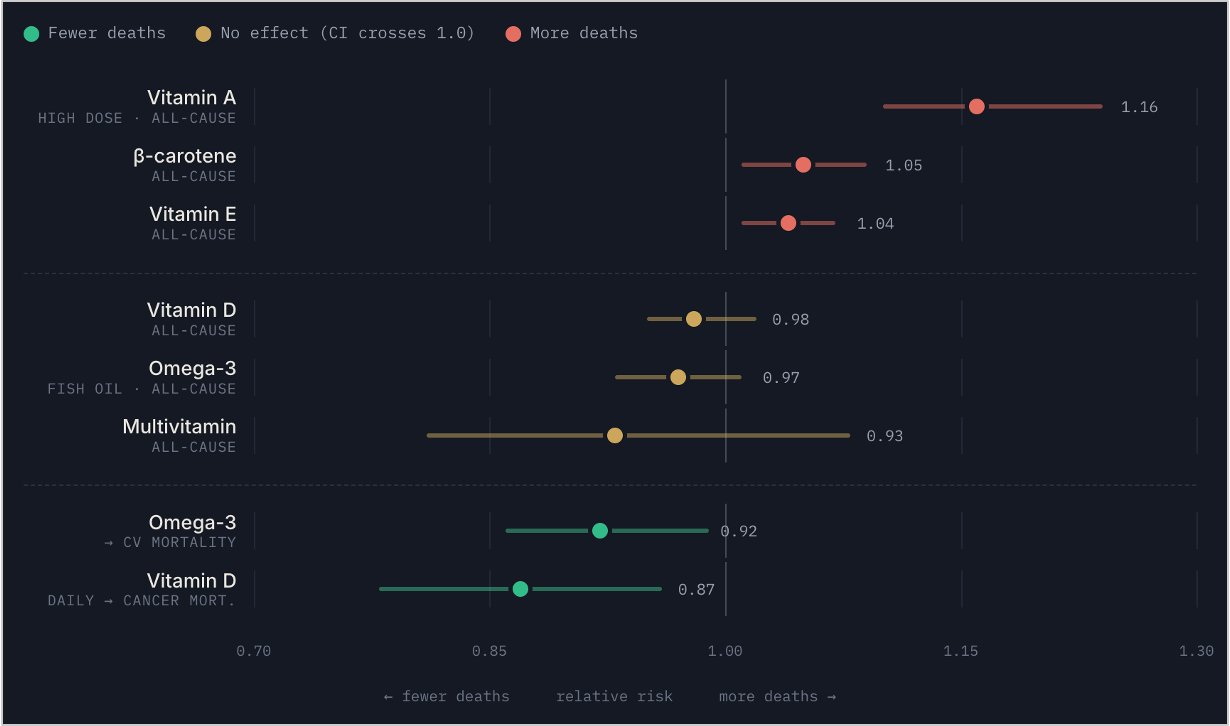
I'll keep this one short, because the evidence is brutal – and I say this as someone who used to take about 50 pills a day. When you look at randomized controlled trials on whether supplements change mortality rates, most do nothing. Even worse, some of them are actively harmful (vitamin A raises mortality).
Omega-3 and Vitamin D have the least-discouraging data. Neither supplement shows an all-cause mortality reduction in RCTs, however omega-3 might help reduce heart attacks in individuals with low levels, and vitamin D might help reduce cancer-related mortality. So the move is simple: test your levels, supplement if you're low on vitamin D or omega-3, skip the rest.
Drugs
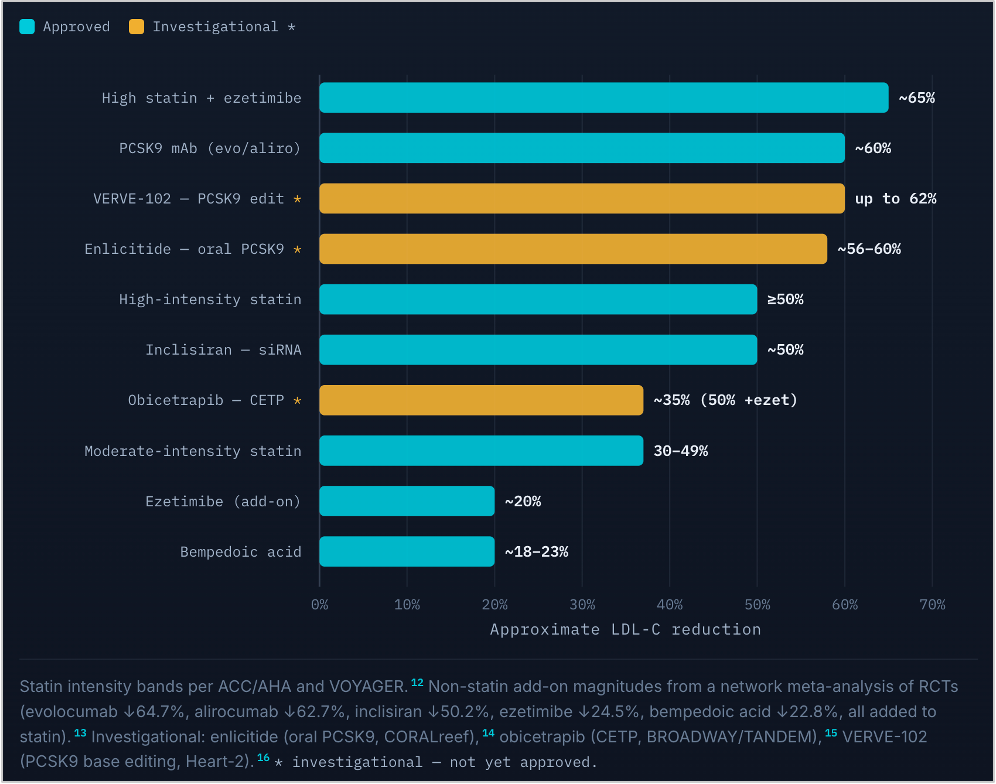
Lowering LDL significantly reduces cardiovascular risk, and statins can cut down LDL levels by around 65%. One thing to note is that while they reliably reduce heart disease, very high dose statins can lead to increased insulin resistance and a higher risk of type 2 diabetes; check with a cardiologist before taking them (source, source).
For a lot of people, an even better drug than a statin is a PCSK9 inhibitor. PCSK9 is a gene discovered through people who naturally have very low cardiovascular risk; drugs that target it lower LDL by around 60% without the metabolic baggage of statins. The underlying science is about two decades old, and the drugs have roughly a decade of real-world use with a clean safety profile so far — though the honest caveat is that "so far" is much shorter than the ~60-year track record behind statins.
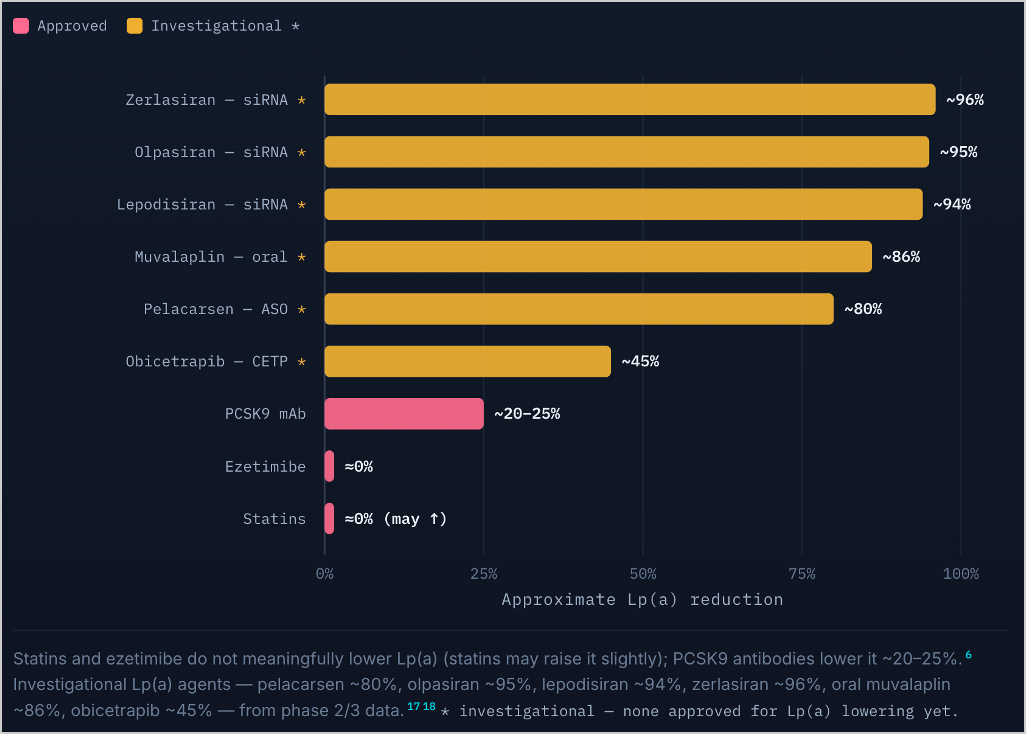
The most exciting frontier is Lp(a). We long assumed it was untouchable genetics, but a new class of RNA-based drugs is showing reductions of up to ~96% in early trials. Very early days, but potentially a big deal for the single largest genetic driver of heart disease.
One more worth mentioning:
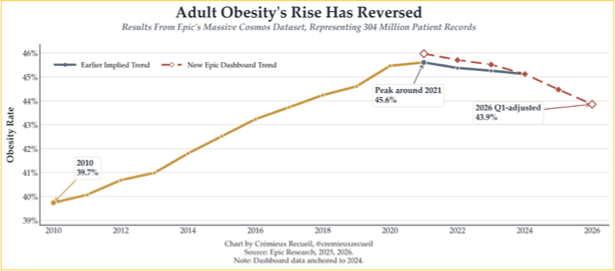
GLP-1s. Whatever you think of them, obesity is bad for you. And for the first time in US history, the obesity rate is flattening, and may even be falling (source, source).
Above all: don't smoke
If you ignore everything else in this post, keep this one. Smoking is behind roughly a third of all cancer deaths, and not just lung cancer, but bladder, liver, gallbladder, stomach, and esophagus too.
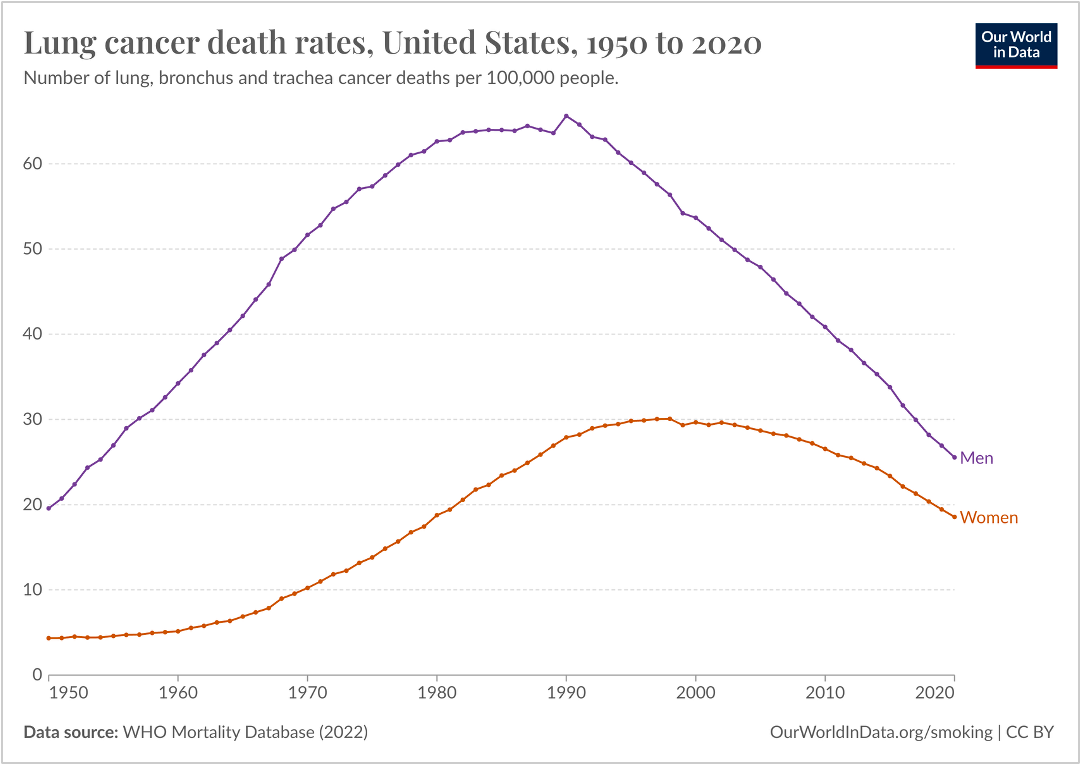
Lung-cancer death rates peaked around 1990 and fell mainly because smoking prevalence dropped after the Surgeon General's report that smoking is, indeed, bad for you. Quitting lowers your risk of cancer, heart disease, diabetes, and stroke more than everything else on this list combined.
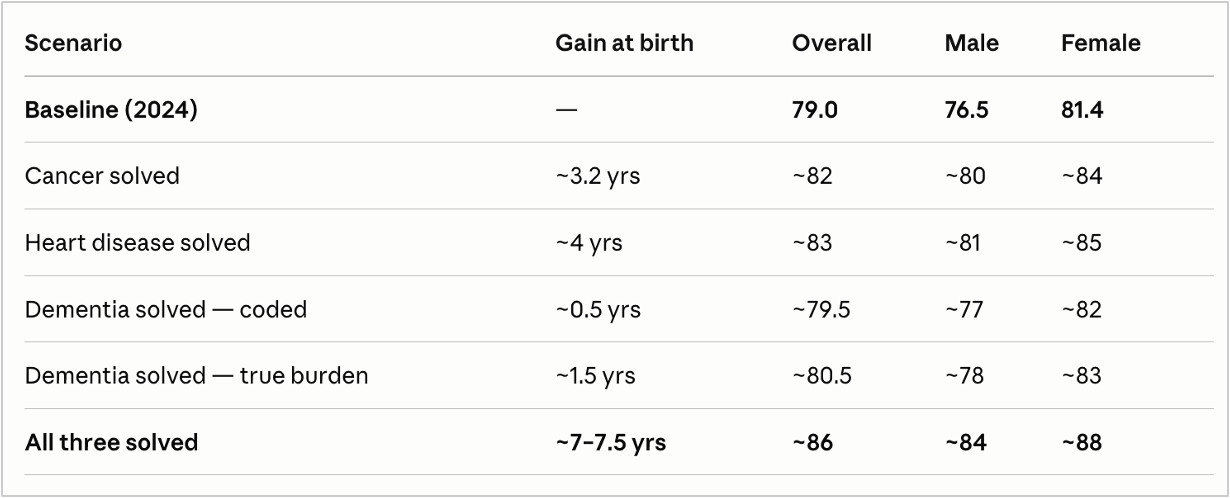
Making cancer and heart disease non-lethal, and delaying dementia, could add roughly 7.5 years of lifespan — enough to push much of the developed world from the high 70s and low 80s toward 86 or 88 (for women). Not through some exotic breakthrough or new drug, but through early detection and a handful of unglamorous habits and drugs.
So the whole protocol, in one breath: measure the things that matter, don't smoke, exercise most days, eat real food, take almost no supplements, and lower your LDL if it's high. Everything else is optimization around the edges.
Getting to 100
But how about getting to 100, which is where we started? Can we actually get to 100 healthy years for everyone?
Making the big three diseases we've covered non-lethal gets us into the high 80s. Now let's look at what actually kills the people who make it past 80, and see if there's anything we can do about it.
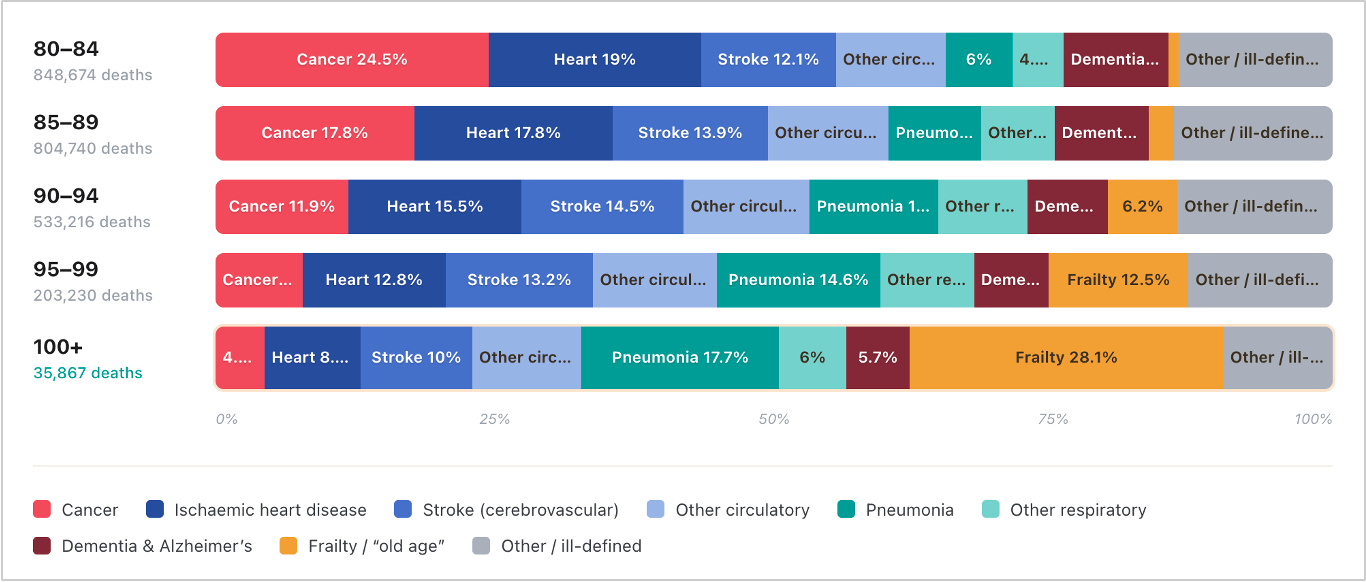
The answer changes as you climb the age curve. From 80 to 100 it's still mostly cancer, heart disease, and increasingly strokes – the same enemies, so the protocol above still applies. But in the mid-90s and beyond, something very different takes over: frailty and pneumonia. These are related, for reasons we'll explore shortly.
Frailty gets written on death certificates as "old age," but underneath it's really four distinct things.
Sarcopenia: the loss of muscle and physiologic reserve. As muscle and your ability to withstand stressors fade, an ordinary infection or fall becomes something you can't bounce back from. This is the target of much of the geroscience work: senolytic drugs, muscle stem-cell treatments, metabolic interventions.
Immunosenescence: the aging of the immune system. A worn-down immune system turns a routine lung infection into a final event, which is why pneumonia kills so many of the very old. The target here is immune rejuvenation: better vaccines, thymic regeneration, and infection prevention designed specifically for the oldest patients.
Cardiac amyloidosis: wild-type ATTR is an age-related amyloid plaque that stiffens the heart, found in roughly 70% of autopsied supercentenarians. It usually gets miscoded as ordinary heart disease, but it isn't – it's a distinct and increasingly treatable condition. We already have drugs like tafamidis, plus gene silencers that knock down the protein driving ATTR, so this is totally solvable already.
Organ failure and sepsis: the single-organ collapses (kidney failure being the classic) that cascade into the whole system shutting down. This is the messy "everything else" bucket of old-age death.
So can we solve frailty?
Three research directions are showing real promise. Let's first look at the science, then cover what I expect to happen in the next decade versus 20-30 years.
Epigenetic reprogramming. The idea is to reset the epigenetic marks that drift as cells age, rejuvenating tissue without touching the underlying DNA. Near-term, the work is organ-specific: companies like Life Biosciences (in the eye) and NewLimit (in the liver) are trying to rejuvenate one tissue at a time (source, source). The hope is systemic reprogramming: rejuvenating muscle, immune, and organ tissue across the whole body. The honest catch with this direction is controllability and cancer risk; these are real unsolved problems, because the same machinery that rejuvenates a cell can also nudge it toward becoming a tumor (source).
In-vivo gene and cell editing. We're close to a single dose of CRISPR that knocks down the protein driving cardiac amyloid by ~90%. This is not science fiction, it's in trials now (source). Further out, the ambition is using CRISPR for multiplexed edits that correct the accumulated somatic mutations we all pick up with age – essentially repairing genomic damage as it builds.
Senolytics. The goal here is to clear out the senescent zombie cells that accumulate with age and drive chronic inflammation. It's still an unproven direction (trials are ongoing) – the long-term vision is precision senotherapy tuned to specific tissues and cell types, giving you continuous, personalized protection against aging (source, source).
What I actually think happens
To be clear, a lot of these initiatives are big and unproven bets, so I'll flag my confidence rate as I go.
Within the next decade, I'd put real money on a few things. One: cardiac amyloidosis becoming controllable; between approved stabilizers, gene silencers in late-stage trials, single-dose CRISPR knockouts, and plaque-clearing antibodies, we're nearly there. Two: muscle loss getting its first real drug – myostatin or activin inhibitor paired with a GLP-1, defending muscle in both the old and the (now very many) people losing weight on GLP-1s. Three: pig-kidney transplants moving into routine trials for kidney disease. And four: early thymic-regeneration protocols aimed at rebuilding the immune system.
Within 20–30 years, these are the harder, higher-payoff bets: restoring physiologic reserve through reprogramming and stem-cell work (still first-in-human and preclinical today), rebuilding the immune system through thymus regrowth and blood stem-cell resets (early, and durability is unproven), and lab-grown autologous organs – growing you a new organ from your own cells. These are the moonshots. I don't know which will pan out, but I'd be surprised if none of them did.
Where this leaves us
We now understand cancer and heart disease well enough to make them non-lethal within the next two decades, through early detection and better treatment. We can predict dementia decades ahead and start delaying it with lifestyle changes. We have a growing toolkit – data, diet, supplements, drugs – to push these diseases into the non-lethal category. And for the first time, we're taking a serious run at frailty itself, the final frontier.
Solving frailty is what takes us from the high 80s to 100 healthy years. We're not there yet, and I don't want to oversell timelines on science that's mostly still in trials and labs. But between the protocol you can start today and what's coming down the pipe, it's a great time to be growing old.
To 100 healthy years!